February 2024
Introduction
Human Rights Watch welcomes the opportunity to provide input to the United Nations Human Rights Committee (the “Committee”) ahead of its upcoming review of Indonesia. This submission draws primarily on Human Rights Watch’s research on the situation of people with disabilities at home as well as in faith-healing centers, residential care institutions, and psychiatric hospitals across Indonesia from 2014 to 2020. It proposes issues and questions that Committee members may wish to raise with the government of Indonesia. We hope it will inform the Human Rights Committee’s assessment of the Indonesian government’s compliance with the International Covenant on Civil and Political Rights (ICCPR).
In 2016, Human Rights Watch published a 74-page report, “Living in Hell: Abuses against People with Psychosocial Disabilities in Indonesia,” documenting abuses faced by people with disabilities, including children, in Indonesia, including stigma, arbitrary and prolonged detention, involuntary treatment, chaining or shackling, physical and sexual violence, as well as forced contraception. At the time, Human Rights Watch documented 175 cases of shackling and obtained evidence of another 200 documented cases.
In 2018, following additional research, Human Rights Watch published an updated report, “Indonesia: Shackling Reduced, but Persists,” noting the positive steps taken by the Indonesian government to tackle shackling. The Indonesian government rolled out a nationwide outreach program to collect data, raise awareness, and provide community-based services, including mental health care.
A 2020 Human Rights Watch global report, “Living in Chains: Shackling of People with Psychosocial Disabilities Worldwide,” found that despite government efforts, the practice of chaining persisted in Indonesia and people with psychosocial disabilities continued to be arbitrarily detained in psychiatric hospitals, residential care institutions, and faith-healing centers where they face abuse.
Right to Equality and Non-discrimination (art. 2)
The 1945 Constitution of Indonesia guarantees fundamental rights to all its citizens. Although the constitution does not explicitly refer to persons with disabilities, it lays the foundation for other disability rights laws and provides the legal basis against discrimination.[1]
Indonesia’s Mental Health Act (MHA) of 2014 contains provisions for reducing stigma and bias against persons with psychosocial disabilities, and accountability for abuses including pasung (meaning to “tie” or “bind”).[2] Problematically, however, the law adopts a pejorative view of persons with psychosocial disabilities as people who have “obstacles in carrying out the functions of the human being,” who as such may be subjected to “coercive” rehabilitation.[3] It allows them to be stripped of legal capacity, without due process, including the right to make their own medical decisions.[4] Both of these provisions often lead to abusive treatment.
Shackling of Persons with Psychosocial Disabilities (arts. 7, 9, 10, 12)
In Indonesia, the widespread practice of pasung refers to the physical restraint of persons with real or perceived psychosocial disabilities, within the home or just outside.[5] Pasung is typically practiced by families who believe that the relative with the psychosocial disability is possessed by evil spirits, or are worried that the person might hurt themselves or others, or might run away. Pasung is also practiced by faith-healers in religious institutions as a form of punishment or “treatment” and by staff in care institutions. The continued practice and the government’s failure to take effective action constitutes serious violations of several rights found in the ICCPR.
Cruel, inhuman or degrading treatment, involuntary medical treatment (art. 7, GC 20)
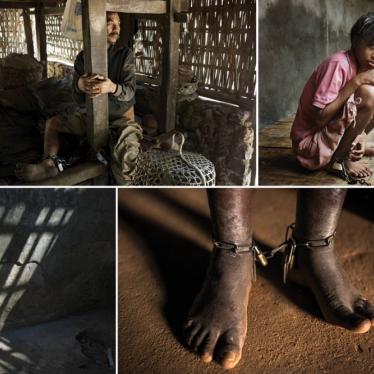
Pasung in Indonesia consists of chaining people or locking them in a room, shed, cage, or animal enclosure (including chicken coops, pig pens, and goat sheds) for periods ranging from hours to days, to years. The nature of shackling means people may not be able to stand or move at all, leading to long-term physiological damage and psychological trauma.
Research by Human Rights Watch globally has found that a person who is shackled can be affected by post-traumatic stress, malnutrition, infections, nerve damage, muscular atrophy, and cardiovascular problems.[6] In Indonesia, people who were shackled had no movement beyond the length of the chain – usually about two meters, having to bathe, defecate, urinate, and sleep within the radius where they were chained.[7]
Human Rights Watch met a 52-year-old woman with a psychosocial disability who was rescued by community health workers in Cijeruk, Bogor. “We locked her in her room for five years,” her sister said. “She would sleep on the floor; she couldn’t walk because her muscles had stopped working. We gave her a bucket to urinate and defecate in. It was very smelly. It made me very sad.” The family felt they had no alternative but to lock her up. But after a visit and help from outreach workers, her sister said, she was released and is now receiving support in the community.[8]
Pasung can also be a temporary measure that is used to restrain a person with a psychosocial disability for shorter time periods while the family goes out to work or when the person is having a crisis. In religious healing centers, it is used as a form of restraint, punishment, or “treatment.” In the case of private institutions and healing centers, the management may have an incentive to detain people as they are paid by the family. In many countries, including Indonesia, this is a profitable business.
In faith-healing centers, Human Rights Watch documented that persons with real or perceived psychosocial disabilities were routinely forced to take medication or alternative “treatments” (such as vigorous, painful massages and baths), without their consent.
Informed consent is a bedrock principle of medical ethics and international human rights law, and forcing individuals to take medicines without their knowledge or consent violates their rights.[9] The UN Special Rapporteur on torture has noted that “involuntary treatment and other psychiatric interventions in health-care facilities” can be forms of torture and ill-treatment.[10] In addition, the UN Special Rapporteur on violence against women has condemned forced psychiatric treatment as a form of violence.[11] In her 2018 report, the UN Special Rapporteur on the rights of persons with disabilities called on states to ensure that all health-related services “include a human rights-based approach to disability, are non-discriminatory, seek informed consent prior to any medical treatment, respect privacy and are free from torture or other cruel, inhuman or degrading treatment.”[12]
Patients with psychosocial disabilities in government and privately run mental hospitals are also routinely forced to take medication, locked in isolation rooms, and subject to involuntary treatment ranging from physical and chemical restraints to unmodified electroconvulsive therapy (ECT).[13] Former UN Special Rapporteur on torture, Manfred Nowak, has noted that unmodified ECT (without anesthesia, muscle relaxants, and oxygen) is an unacceptable medical practice that may constitute torture or ill-treatment, as it may cause adverse effects such as cognitive deficits and loss of memory.[14]
Human Rights Watch documented 25 cases of physical violence including beatings and six cases of sexual violence, a lack of respect for privacy and dignity while bathing, and chaining children, women, and men close together – putting women and girls at risk of sexual violence.[15] Furthermore, Human Rights Watch documented 22 cases of forced seclusion, including of children, ranging from a few hours to over a month. In addition, in government as well as privately run residential care institutions, we found evidence of staff giving women contraception without their consent or knowledge.
Arbitrary detention, respect for inherent human dignity (arts. 9, 10, GC 8.1)
State-run residential institutions and private faith-healing centers where people with disabilities are arbitrarily detained are exceptionally overcrowded, unsanitary, and lack measures to support personal hygiene.[16]
Under Indonesian law, it is relatively easy to involuntarily admit a person with a psychosocial disability to an institution. The Mental Health Act (2014) allows a family member or guardian to admit a child or an adult with a psychosocial disability without their consent to a mental health or a social care institution, and without any judicial review. Human Rights Watch found 65 cases of people arbitrarily detained in mental hospitals, social care institutions, and nongovernmental organization-run or traditional or religious centers. None of those with psychosocial disabilities interviewed by Human Rights Watch who were living in institutions said that they were there voluntarily.[17]
In 2015, the UN Special Rapporteur on torture explicitly stated that shackling “unequivocally amount[s] to torture even if committed by non-State actors under conditions in which the State knows or ought to know about them.”[18] In her 2019 report, the UN Special Rapporteur on the rights of persons with disabilities stressed that “States must protect persons with disabilities against home-based deprivation of liberty, including home confinement, shackling and pasung.”[19]
In 2022, following the initial report of Indonesia, the UN Committee on the Rights of Persons with Disabilities expressed concern “about deprivation of liberty on the basis of impairment, in particular for persons with psychosocial disabilities or intellectual disabilities” and explicitly referred to shackling, seclusion, and restraints as harmful practices.[20] The Committee called on the Indonesian government to “prohibit the use of shackling, seclusion and all forms of restraints in all settings, including within families and in social care institutions, and develop and promote non-coercive, community-based mental health supports and services.”[21]
Progress
Human Rights Watch’s 2018 follow-up report, “Indonesia: Shackling Reduced, But Persists,” documents the important steps taken by the Indonesian government to end the practice of shackling people with psychosocial disabilities and expand community-based mental health services.
At the time, Human Rights Watch found that the number of people with psychosocial disabilities who were shackled or locked up in confined spaces had dropped from nearly 18,800 in 2016 to about 12,800 in July 2018, according to Indonesian government data.[22] The change resulted in part from a community outreach program to over 16.2 million households. Despite this progress, Human Rights Watch found that people with psychosocial disabilities continued to be detained arbitrarily in faith-healing centers, social care institutions, and mental hospitals.
Ratih, a woman with a psychosocial disability who had been detained for several years in the Yayasan Galuh Rehabilitation Center, a privately run institution on the outskirts of Jakarta, in Bekasi, said: “I have been chained here three times. The staff told me I was handcuffed for my own benefit. I got hit by the staff and was handcuffed for one whole week. I couldn’t even go to the toilet, I had to pee there, in my clothes. I had to ask my friend to help me eat but she was too scared [of the staff]…. I want to go home, I don’t belong here.”[23]
The Indonesian government officially banned pasung under law in 1977. However, the practice remains to this day. It is estimated that 57,000 people with psychosocial disabilities in Indonesia, including children, have been shackled at least once in their lives with approximately 15,000 still living in chains as of November 2019.[24] In many countries, including in Indonesia, Covid-19 disrupted basic services, leading to people being shackled for the very first time or returning to life in chains after having been released.
According to a 2023 media report, seven people with psychosocial disabilities who were shackled died over a three-months period on Flores Island.[25]
In 2023, the Indonesian Mental Health Association petitioned the Constitutional Court of Indonesia to review article 433 of the Civil Code to ban guardianship of people with psychosocial or intellectual disabilities. In July 2023, in an important step forward, the Constitutional Court partially granted the petitioners’ request by altering the nature of guardianship of people with disabilities from being mandatory to being optional.
Human Rights Watch encourages the Committee to ask the Indonesian government:
- Is there official data on the number of people who are currently shackled in Indonesia?
- What steps has the government taken to eliminate the practice of shackling of people with psychosocial disabilities?
- How many children with psychosocial disabilities are currently arbitrarily detained in faith-healing centers, government-run as well as private residential care institutions, and psychiatric hospitals across Indonesia?
- What steps has the government taken to end the arbitrary detention of people with psychosocial disabilities in psychiatric hospitals, residential care institutions, and faith-healing centers?
- What concrete steps has the government taken to ban all forms of involuntary treatment, including ECT, without the person’s free and informed consent?
- What steps has the government taken to develop adequate, quality, and voluntary community-based support and mental health services?
Human Rights Watch asks the Committee to consider including the following recommendations in its concluding observations on Indonesia:
- Strengthen and monitor the implementation of laws banning pasung.
- Recognize institutionalization based on the existence of a disability as a form of discrimination and without consent of the individual as a form of arbitrary detention.
- Ban all forms of involuntary treatment, including ECT, without the person’s free and informed consent and in all circumstances involving children. Explicitly prohibit the use of seclusion and prolonged restraint. Define exceptional circumstances in which a patient may be considered temporarily unable to give free and informed consent and, in such circumstances, immediate medical treatment may be administered as it would be to any other patient without a disability incapable of consenting to treatment at that moment, provided that the treatment is strictly necessary to address a life-threatening condition or a condition of similar gravity.
- Develop a time-bound plan to shift progressively to community-based mental health, support, and independent living services.
- Create and implement a de-institutionalization policy and a time-bound action plan for de-institutionalization, based on the values of equality, independence, and inclusion for persons with disabilities.
- Ensure that people who have been released from state and private institutions have access to psychosocial support and social services. Children should have access to child psychologists and special support services.
- Progressively develop voluntary and accessible community-based mental health support services, in consultation with people with psychosocial disabilities and with the support of international donors and partners. This should include the development of psychosocial support services and integration of mental health services in the primary healthcare system.
- Amend or repeal all domestic legislation that is contrary to the Convention on the Rights of Persons with Disabilities to ensure that persons with psychosocial or intellectual disabilities are guaranteed legal capacity, equal recognition before the law, supported decision-making as opposed to guardianship (plenary and limited), freedom from discrimination, and protection from arbitrary detention and treatment.
- Conduct regular, unannounced monitoring visits to government and private social care institutions as well as faith-healing centers, with unhindered and confidential interaction with both staff and patients, and report publicly on the findings from these visits.
- Train and sensitize government health workers, mental health professionals, and staff in institutions to the concerns and needs of persons with psychosocial disabilities, including children, and create a confidential and effective complaint mechanism for individuals with psychosocial disabilities to report abuse.
- Conduct extensive public awareness and information campaigns including through the media, religious groups, and schools on mental health conditions, the rights of persons with disabilities, and alternatives to institutionalization and restraint.
[1] Human Rights Watch, Living in Hell: Abuses against People with Psychosocial Disabilities in Indonesia, March 20, 2016, https://www.hrw.org/sites/default/files/report_pdf/indonesia0316web.pdf, pp. 68-69.
[2] Mental Health Act, 2014, art. 86.
[3] Ibid., arts. 2, 28.
[4] Ibid., arts. 21, 70, 71, 72.
[5] Ibid.
[6] Human Rights Watch, Living in Chains: Shackling of People with Psychosocial Disabilities Worldwide, October 6, 2020, https://www.hrw.org/sites/default/files/media_2020/10/global_shackling1020_web_2.pdf, p. 49.
[7] Ibid., p. 45.
[8] “Indonesia: Shackling Reduced, But Persists,” Human Rights Watch news release, October 2, 2018, https://www.hrw.org/news/2018/10/02/indonesia-shackling-reduced-persists.
[9] International Covenant on Civil and Political Rights (ICCPR), adopted December 16, 1966, G.A. Res. 2200A (XX1), 21 U.N. GAOR Supp. (No. 16) at 52, U.N. Doc. A/6316 (1966), 999 U.N.T.S. 171, entered into force March 23, 1976. Indonesia ratified the ICCPR in 2006. International Covenant on Economic, Social and Cultural Rights (ICESCR), adopted December 16, 1966, G.A. Res. 2200A (XXI), 21 U.N. GAOR Supp. (No. 16) at 49, U.N. Doc. A/6316 (1966), 993 U.N.T.S. 3, entered into force January 3, 1976, art. 12. Indonesia ratified the ICESCR in 2006. See also, Beijing Declaration and Platform for Action, Fourth World Conference on Women, September 15, 1995, A/CONF.177/20 (1995), art. 108(e); United Nations Educational, Scientific, and Cultural Organization (UNESCO), Universal Declaration on Bioethics and Human Rights, adopted October 2005, SHS/EST/05/CONF.204/3 REV, arts. 6 and 9; UN Committee on Economic, Social and Cultural Rights, General Comment 14, The right to the highest attainable standard of health (Twenty-second session, 2000), U.N. Doc. E/C.12/2000/4 (2000), U.N. Doc. HRI/GEN/1/Rev.6 at 85 (2003), para. 8; UN Office of the High Commissioner for Human Rights/WHO, FactSheet No. 31, The Right to Health, http://www.ohchr.org/Documents/Publications/Factsheet31.pdf, pp. 16-18.
[10] UN Commission on Human Rights, Report of the Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment, Juan E. Méndez, A/HRC/22/53, February 1, 2013, http://www.ohchr.org/Documents/HRBodies/HRCouncil/RegularSession/Session22/A.HRC.22.53_English.pdf (accessed December 28, 2013), para. 64.
[11] UN Commission on Human Rights, Report of the Special Rapporteur on violence against women, its causes and consequences, A/67/227, August 3, 2012, http://www.ohchr.org/Documents/Issues/Women/A.67.227.pdf (accessed December 10, 2013), pp. 10, 13.
[12] UN General Assembly, Report of the Special Rapporteur on the rights of persons with disabilities, A/73/161, July 16, 2018, https://undocs.org/en/A/73/161 (accessed September 17, 2020), para. 74(e).
[13] Ibid., pp. 46-58.
[14] UN General Assembly, Interim report of the Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment, A/63/175, July 28, 2008, https://documents-dds-ny.un.org/doc/UNDOC/GEN/N08/440/75/PDF/N0844075.pdf (accessed July 28, 2022), para. 50.
[15] Human Rights Watch, Living in Hell, https://www.hrw.org/sites/default/files/report_pdf/indonesia0316web.pdf, p. 12.
[16] Ibid., p. 45.
[17] Ibid., p. 6.
[18] UN Human Rights Council (UNHRC), Follow-up report of the Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment on his follow-up visit to the Republic of Ghana, A/HRC/31/57/Add.2, February 25, 2015, https://undocs.org/en/A/HRC/31/57/Add.2 (accessed February 10, 2022).
[19] UNHRC, Report of the Special Rapporteur on the rights of persons with disabilities, A/HRC/40/54, January 11, 2019,
https://undocs.org/en/A/HRC/40/54 (accessed July 28, 2022), para. 52.
[20] UN Committee on the Rights of Persons with Disabilities, Concluding observations on the initial report of Indonesia, CRPD/C/IDN/CO/1, October 12, 2022, https://tbinternet.ohchr.org/_layouts/15/treatybodyexternal/Download.aspx?symbolno=CRPD%2fC%2fIDN%2fCO%2f1&Lang=en (accessed December 14, 2023), paras. 34, 36.
[21] Ibid., para. 37.
[22] “Indonesia: Shackling Reduced, But Persists,” Human Rights Watch news release, October 2, 2018, https://www.hrw.org/news/2018/10/02/indonesia-shackling-reduced-persists.
[23] Ibid.
[24] Human Rights Watch, Living in Chains, https://www.hrw.org/sites/default/files/media_2020/10/global_shackling1020_web_2.pdf; Living in Hell, https://www.hrw.org/sites/default/files/report_pdf/indonesia0316web.pdf, p. 35; Ministry of Health of Republic of Indonesia, “Stop Stigma and Discrimination to People with ‘Mental Disorder’,” October 10, 2014, http://www.depkes.go.id/article/view/201410270011/stop-stigma-dan-diskriminasi-terhadap-orang-dengan-gangguan-jiwa-odgj.html (accessed August 20, 2015); Marsel Rombe, “Indonesian Mental Health Law Passed after Five Years,” Jakarta Globe, July 13, 2014, http://jakartaglobe.beritasatu.com/news/indonesian-mental-health-law-passed-five-years (accessed August 19, 2015).
[25] Ditulis Oleh Pater Avent Saur SVD, “Ketika Napas Berakhir di Pasungan,” Krebadia, October 1, 2023, https://krebadia.com/ketika-napas-berakhir-di-pasungan/ (accessed December 14, 2023).